The evidence is mounting from frontline caregivers dealing with Covid19 patients. Previous posts provide examples of HCQ treatment along with other proven medicines (eg. Azithromycin) and supplements (eg. Zinc. vitamins C and D). Summarized in the chart above is the role of HCQ+ according to the progression of the disease Covid19.
HCQ Prevents Covid19
The first column on the left is sometimes called PrEP, or pre-exposure to the virus SARS CV2. Now we are getting studies confirming that HCQ plays an important prophylactic role in blocking the virus from taking hold when someone is infected. The Times of India June 19, 2020, article is HCQ beneficial as preventive drug: SMS doctors told ICMR. Excerpts in italics with my bolds
JAIPUR: Sawai Man Singh Hospital was the first to use hydroxychloroquine (HCQ) and anti-HIV drugs — Lopinavir and Ritonavir — to treat the first few Covid-19 patients besides using the combination as a preventive drug on others.
More than 4,300 healthcare workers including doctors and nurses have been given HCQ to help them prevent the infection as there are high chances of them getting infected while treating Covid patients.
“As far as prophylaxis is concerned, more than 4,300 doctors and health works were given HCQ as approved by Indian Council of Medical Research (ICMR) out of which around 45 health persons tested positive and recovered later,” said Dr Sudhir Bhandari, principal and controller, SMS Medical College.
The hospital claimed that preventive treatment approach at SMS Hospital has been very rewarding and results of these have been shared with ICMR.
“We have used these drugs with perfect scientific background and proven efficacy in SARS Cov-2 Infection and SMS Medical College created a bridge between point of no specific treatment till the specific drug treatment is established. All these drugs were part of solidarity trial by WHO of which SMS Hospital is a centre,” said Bhandari.
SMS Hospital was declared as non-Covid hospital on June 1. But before that, it emerged as a role model of management of Covid patients. From the very beginning, 300 ICU beds and more than thousand IPD beds were dedicated for Covid patients. A separate Covid OPD and observation wards for suspects was created at Charak Bhawan. Also, 28 wards were created for Covid patients of different categories. For critically ill patients, Infectious Disease Hospital (IDH) was fully equipped with ICU facilities.
During the peak of the pandemic, average 500 plus patients were admitted to SMS from asymptomatic category to severe category.
Number of faculty was put on floor duty, which included consultants from the department of medicine and anaesthesia. Resident doctors were doing duty in each shift and hundreds of nursing, paramedics and technicians were on round-the-clock duty.
Only studies comparing a group of COVID19 patients treated with a chloroquine derivative to a control group without chloroquine derivatives were included. Non-comparative (single arm) studies and studies comparing two groups treated with chloroquine derivatives at different dosages or with different delay of treatment were excluded. Studies were classified as “big data” studies when conducted on electronic medical records extracted by public health specialists and epidemiologists who did not care COVID106 19 patients themselves. Conversely, studies were classified as “clinical studies” when mentioning details of treatments (dosages, duration, contraindications, monitoring…) and conducted by authors physicians (infectious diseases and internal medicine specialists, and pulmonologists) who cared for COVID-19 patients themselves.
Twenty studies were identified involving 105,040 patients (19,270 treated patients) from nine countries (Brazil, China, France, Iran, Saudi Arabia, South Korea, Spain, and USA). Big data observational studies were associated with conflict of interest, lack of treatment dosage and duration, and absence of favorable outcome. Clinical studies were associated with favorable outcomes and details on therapy. Among clinical studies, three of four randomized controlled trials reported a significant favorable effect.
Among clinical studies, a significant favorable summary effect was observed for duration of cough (Odds ratio (OR), 0.19, p = .00003), duration of fever (0.11, p = .039), clinical cure (0.21, p = .0495), death (0.32, p = 4.1×10-6) and viral shedding (0.43, p = .031). A trend for a favorable effect was noted for the outcome “death and/or ICU transfer” (0.29, p = .069) with a point estimate remarkably similar to that observed for death (∼0.3). In conclusion, a meta-analysis of publicly available clinical reports demonstrates that chloroquine derivatives are effective to improve clinical and virological outcomes but, more importantly, it reduces mortality by a factor 3 in patients infected with COVID-19.
All “big data” studies reported a lack of beneficial effect of the treatment and were significantly more likely associated with “Cons” variable (5/5 vs 3/15, p = .004). This was also observed by examination of the meta-analysis forest plot (Figure 2, Table S3 to S8). In addition, both “conflicts of interest” (p = .01) and “not described treatment protocol” variables (p = .004) were associated with “Cons” variable. Conversely, clinical studies were more likely to report a favorable effect of chloroquine derivatives in COVID-19 patients (p <.05). Consistently, clinical studies with detailed treatment protocol were more likely associated with the observation of a favorable effect of the treatment (p < .05).
In the big data analyses, 4 comparisons reported a significant effect, and all were deleterious (4/4). In the clinical studies, 17 comparisons reported a significant effect, and all were beneficial.
A Henry Ford Health System study shows the controversial anti-malaria drug hydroxychloroquine helps lower the death rate of COVID-19 patients, the Detroit-based health system said Thursday.
Officials with the Michigan health system said the study found the drug “significantly” decreased the death rate of patients involved in the analysis.
The study analyzed 2,541 patients hospitalized among the system’s six hospitals between March 10 and May 2 and found 13% of those treated with hydroxychloroquine died while 26% of those who did not receive the drug died.
Among all the patients in the study, there was an overall in-hospital mortality rate of 18%, and many who died had underlying conditions, the hospital system said. Globally, the mortality rate for hospitalized patients is between 10% and 30%, and 58% among those in the ICU or on a ventilator.
“As doctors and scientists, we look to the data for insight,” said Steven Kalkanis, CEO of the Henry Ford Medical Group. “And the data here is clear that there was a benefit to using the drug as a treatment for sick, hospitalized patients.”
During the current COVID-19 epidemic, most of the evidence is collected by treating physicians, most of whom do not report their results in peer reviewed journals. Hence, there appears to be an especially broad gap between field experience and academic coverage of hydroxychloroquine-based COVID-19 treatments. The objective of this study is to bring field evidence into the academic literature.
Four relevant, non-academic surveys of physicians, in the US and globally, have been identified and checked for quality, statistical significance, coverage, and conflicts of interest. To avoid uninformed and unduly influenced opinions, only surveys conducted from April 4 to April 19 have been considered. These surveys were answered by thousands of physicians, who treated tens of thousands of COVID-19 patients.
The results: 85% of doctors said that hydroxychloroquine is at least somewhat effective for COVID-19. Hydroxychloroquine was the most utilized treatment for COVID-19 patients. 35%-40% of the doctors using the drug called it very effective or extremely effective against COVID-19. 65% of doctors said they would prescribe hydroxychloroquine for COVID-19 to their family members.
The author declares no competing interest.
No funding was provided for this work.
All relevant ethical guidelines have been followed.
Introduction
The largest body of knowledge of COVID-19 treatments is collected by practicing physicians, outside of research settings, and not reported in peer reviewed publications. The objective of this systematic review is to capture some of this clinical experience and bring it into the academic literature. The scope is limited to hydroxychloroquine-based treatments, administered in the early (viral) stages of COVID-19.
The most effective and popular COVID-19 treatment regimen, combining hydroxychloroquine with azithromycin, was introduced by Institut Hospitalo-Universitaire (IHU) Méditerranée Infection, directed by Didier Raoult. The HCQ based treatment was presented at a March 16, 2020 conference (Raoult, 2020), and published a few days later as (Gautret, et al., 2020). It became instantly popular among physicians on March 20-21.
Many doctors and hospitals used this treatment from March 20 to March 27. The treatment’s effects were observed and discussed with colleagues, from March 27 to April 4. Thus, starting around April 4, doctors who used or observed the use of any HCQ-based treatment were able to provide eyewitness testimonies. Many other doctors were able to give their expert opinions, based on the experiences of their colleagues and their professional knowledge. On April 20, the NIH COVID-19 Panel published guidelines that were adverse to HCQ treatment (The National Institutes of Health COVID-19 Treatment Guidelines Panel , 2020). On April 24, the FDA issued a warning (The FDA, 2020) concerning the drug’s safety. These events might have prejudiced some doctors against HCQ. The time frame chosen for this systematic review, April 4 to April 19, is selected to ensure that physicians had sufficient experience with HCQ but had not yet been prejudiced by external events.
Explanation of Methods
A physician’s answers to questions regarding the treatment s/he has used can be considered direct evidence. Corresponding statistics computed from the responses of N physicians, treating on average M patients, should have equal power and higher resilience than results of a randomized clinical trial conducted on N*M patients, in the absence of a systematic bias.
A physician’s choice of a certain treatment over another, indicates that the chosen treatment is considered more effective. A physician’s decision to implement a certain treatment rather than no treatment proves that the treatment’s effectiveness/risk profile is considered high enough. This can be considered indirect evidence.
A physician’s opinion about a treatment which he or she did not directly use in practice, but learned about from other physicians, can be considered an expert opinion.
Well implemented surveys can capture much of this evidence and expert opinions.
Methods
Surveys or polls of physicians were sought, using multiple search engines (DuckDuckGo, Bing, Google, Yandex), searching for ‘physician survey hydroxychloroquine’, ‘doctors survey hydroxychloroquine’, and similar combinations of keywords; no quotes; not limited by dates. The search was repeated many times, excluding previously found items.
Surveys or polls from three companies were found. Each of the three survey companies were researched and confirmed as reputable. A list of all relevant surveys and polls, done by these three companies, in the selected time frame, was compiled. This yielded four surveys from three different companies: Sermo (two surveys), InCrowd, and Jackson Coker. Sermo’s surveys appeared to be most professional and informative. No strong competing interests, that may have any bearing on the surveys, were found in any of the three companies.
Drugs used for other effects, other than antiviral, have been excluded from this review for the following reasons. High dose steroids are used during a cytokine storm. Acetaminophen, Ibuprofen, and Herbal remedies are used as symptomatic treatment. Vitamin D is not considered an antiviral treatment or an essential part of one. Bronchodilators are bronchodilators.
Results
Although the surveys posed different questions to different audiences, the results were congruent. Because CQ is hardly used in practice, CQ and HCQ are both referred to as HCQ.
Table 1. Summary of results
J C
Sermo W3
Sermo W4
InCrowd
Polling Date
April 4-7
April 6-9
April 13-15
April 14-15
Publication Date
April 8
April 15
April 23
April 21
Location
USA
Global
Global
USA
# doctors
1271
4016
5500
203
Recommended HCQ
65% (1)
n/a
n/a
n/a
# COVID-19 treaters
n/a
1337
1376 (3)
203
Used HCQ / HCQ+AZ
n/a
50%
53%
n/a
% HCQ users rating VEE (4)
n/a
40%
35%
n/a
Reported HCQ effective
n/a
85% (5)
n/a
n/a
Would give to patients’ %
n/a
n/a
n/a
30% (2)
Remarks
HCQ shortages
Would give HCQ to their family
Would prescribe HCQ / HCQ+AZ to this percentage of their COVID-19 patients, on average. 30% is quite a high number, because most COVID-19 patients probably need no treatment, especially the patients of the surveyed physicians, about a third of whom are pediatricians. The numbers for plasma and Remdesivir are 21% and 16%, respectively.
This number includes physicians who used HCQ in outpatient and hospital ex/ICU settings.
VEE = Very or Extremely Effective (4 or 5 on the scale 0 – 5)
2 or higher on the scale 0 – 5
Notice that except for Jackson Coker, surveys’ results were published about a week after they had been conducted, so their results could not influence each other.
Sermo Week 3
(Sermo W3, 2020)
Survey Period: April 6-9
Published on April 15
Country: Global
N = 4016 – the total number of physicians surveyed, including those who have not treated COVID-19
Effectiveness:
The top treatments used or seen to be used by physicians and reported as very or extremely effective among COVID-19 treaters include:
Table 2. VEE Treatments
Hydroxychloroquine n=875 (40%)
Plasma from recovered patients n=363 (46%)
Percentage of physicians to report that HCQ/CQ is at least partially effective (scoring 2 or higher on the scale 0 – 5) against COVID-19:
Table 3. Physicians rating HCQ/CQ at least partially effective
Global: 85%
US: 81%
Italy: 94%
Spain: 91%
China: 88%
This data suggests that physicians in countries with more than average COVID-19 experience appreciate HCQ more than physicians in countries with less than average experience.
Usage
N = 1337 (the number of COVID-19 treaters out of the 4016 physicians surveyed)
SCREENING: COVID-19 treaters
Table 4. Medications physicians have used to treat COVID-19 patients
Drug
%
Azithromycin or similar antibiotics
58%
Hydroxychloroquine or Chloroquine
50%
Anti-HIV drugs (e.g. Lopinavir plus Ritonavir)
23%
Drugs used to treat flu (e.g., Oseltamivir)
22%
None
16%
Treatments used by less than 10% COVID-19 treaters are excluded here.
The survey did not include inquiries about drug combinations. However, these numbers and well-known information from other sources suggest that in most cases when HCQ or CQ was prescribed, it was in combination with Azithromycin (AZ).
There were important differences in the perceived effectiveness of HCQ in the US as compared to the rest of the world. In the US, HCQ/CQ was used by 39% of COVID-19 treaters, compared to 75% and 83% of practitioners in Spain and Italy, respectively. Of note, Spain and Italy broke the rapid rise and started a rapid decrease in death rates around April 2-3 (Our World in Data, 2020).
Sermo Week 4
(Sermo W4, 2020)
Survey Period: April 13-15
Published on April 23
Country: Global
N = 1376 (after screening; 5,500 doctors were surveyed)
Q11. Effectiveness on patients outside hospital setting (Mild/Moderate): For patients you treat outside the hospital (mild/moderate in community setting), rate the efficacy of medications you have used to treat COVID-19.
Results ordered by the number of physicians who rated the drug Very/Extremely Effective in the more relevant, non-hospital group. (Results are listed only for drugs in Table 6 in the next section) Notice that percentages in parentheses exclude treaters who did not answer the question about each drug’s effectiveness. Effectiveness of HCQ was rated differently in different countries. In the US, it was rated below its rating in the rest of the world.
HCQ / HCQ+AZ is clearly in the league of its own, per number of physicians rating it as “Very or Extremely Effective”.
Usage
N = 1376 (636 / 1045 for Non-Hospital physicians / Hospital physicians, except ICU only)
SCREENING: COVID-19 treaters
Table 6. Share of COVID-19 Treating Physicians Who’ve Used Medication Within Setting
Non-Hospital
Hospital ex/ICU
Computed Average
n=636 (Q8)
n=1,045 (Q9)
Azithromycin
60%
70%
65%
Hydroxychloroquine
40%
66%
53%
Drugs to treat flu
22%
25%
23.5%
Anti-HIV drugs
12%
32%
22%
Vitamin C
28%
21%
24.5%
Zinc
17%
11%
14%
Remdesivir
6%
16%
11%
Plasma
6%
10%
8%
Simple averages have been computed to reflect the higher probability that HCQ-based treatment was started early in non-hospital settings compared with hospital settings.
Given the low standalone effectiveness and broad use of AZ, it is likely that in most cases HCQ was used in combination with AZ. The relatively large percentage for physicians using and highly rating Zinc suggests that HCQ+AZ+Zn was used extensively.
Note 1
33% of treaters complained about HCQ shortages. For comparison, only 27% of the treaters complained about ventilator shortages. The number was 48% for Super Treaters (doctors who treated >20 COVID-19 patients) outside of hospital settings. It is reasonable to conclude that HCQ treatment results would have been even better if not for HCQ shortages, causing treatment delays.
Note 2
This survey captures the relevant results of treating about 25,000 – 30,000 COVID-19 patients (Q7).
InCrowd
(InCrowd, 2020)
Survey Period: April 14-15
Published on April 21
N = 203
Country: USA
Specialties: US Primary Care Physicians (61), Pediatricians (59), and Emergency Medicine or Critical Care Physicians (83)
SCREENING: Physicians who have or are currently treating 20 or more patients with flu like symptoms
Q11: For what percentage of your COVID-19 patient population would you prescribe each of the following treatments? If other, please specify.
Table 7. Surveyed physicians would prescribe to this % of their COVID-19 patients
Drug
%
“Azithromycin etc.”
41%
Hydroxychloroquine or Chloroquine
30%
Plasma
21%
Remdesivir
16%
Antivirals (non-specific)
10%
Flu treatments (e.g. Tamiflu, Xofluza), Anti-HIV Drugs, Interferon-Beta, and Other scored 2%-7% each.
No answers were reported about the combination of drugs, but the numbers suggest that non-pediatric doctors would prescribe HCQ+AZ to ~40% of their COVID-19 patients. Many physicians using HCQ prescribe it only to those deemed at risk, so 30-40% is impressive.
Jackson Coker
(Jackson-Coker, 2020)
Survey Period: April 4-7
Published on April 8
N= 1,271
Country: USA, all 50 states
Reported margin of error is 3% with a 95% confidence level.
SCREENING: None. All physicians who elected to answer the survey, about 1% of the firm’s database of physicians. It was not established whether they treated or did not treat COVID-19 patients. It is likely that there was positive self-selection by doctors who treated COVID-19.
65% said they would prescribe drugs chloroquine or hydroxychloroquine to treat or prevent COVID-19 in a family member. 54% said they would prescribe it early, while another 11% said they would prescribe it if the disease becomes serious. 30% said they would prescribe chloroquine or hydroxychloroquine to a family member prior to the onset of symptoms if they had been exposed to the coronavirus. 11% said they would not use the drug.
73% of physicians practicing solo or with ownership stake in a practice, said they would prescribe HCQ/CQ to a family member. That means that more experienced physicians are more likely to prescribe HCQ. The share drops among critical care, emergency medicine, and hospitalists to 43%, 55%, 54%, respectively.
The lower usage of HCQ by critical care and emergency physicians can be explained by the fact that they are dealing with patients in a later stage of COVID-19, which might be characterized as a different illness, dominated by ADRS and multiple organs damage, rather than by viral infection.
Discussion
Only a small fraction of physicians use plasma, but they highly rate it.
Doctors’ wide-spread use and high recognition of HCQ+AZ treatment against COVID-19 is strong evidence, and, possibly, conclusive proof of the treatment’s safety and effectiveness.
Later Surveys
Sermo’s weekly COVID-19 surveys break the results down by regions, countries, and other useful categories. Sermo continued publishing surveys about doctors’ choices of COVID-19 treatments even after April 19. In May, they reported a decline in the use of CQ/HCQ and a rise in the use of Remdesivir.
InCrowd conducted a similar survey on May 29-31. It also reported a decline in the use of CQ/HCQ and a rise of Remdesivir, possibly for external reasons.
Jackson Coker has conducted no other related surveys.
Remarks
Some doctors started adding Zinc to the HCQ+AZ cocktail, as reported in (Risch, 2020). It is expected that additional experience in treating COVID-19, since the surveyed period, has increased the safety and effectiveness of multiple treatments, including HCQ-based ones.
Conclusions
85% of the globally surveyed physicians recognized HCQ as at least partially effective in treating COVID-19, according to Sermo W3. More than half of the surveyed US physicians would take the drug or give it to family members early or even before onset of symptoms, according to JC.
Aside from the rarely used plasma, HCQ / HCQ+AZ based treatments are preferred by physicians by wide margin over other drugs. HCQ / HCQ+AZ based treatments are the most used, most recommended, and most highly rated by physicians treating COVID-19 at an early stage.
Personal Note
Except for this paragraph, this paper appears here exactly as it was submitted to medrxiv.org on June 30 (MEDRXIV/2020/143800). It was rejected today, on July 4: “We regret to inform you that your manuscript will not be posted. A small number of papers are deemed during screening to be more appropriate for dissemination after peer review at a journal rather than as preprints.“
I felt this might happen when I saw medrxiv’s home page “Supported by Chan Zuckerberg Initiative“. Now, I submit it to an open peer review.
there is an earlier peer-reviewed paper, confirming HCQ+AZ effectiveness:
Jean-Christophe Lagierab, Matthieu Million, Philippe Gautret, Raoult, Didier et al., Outcomes of 3,737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille, France: A retrospective analysis, June 25, Travel Medicine and Infectious Disease https://www.sciencedirect.com/science/article/pii/S1477893920302817
References
FDA. 2020. FDA cautions against use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of heart rhythm problems. fda.gov. April 24, 2020. [Cited: April 24, 2020.] http://archive.is/xwOAc.
Gautret, Philippe , Lagier, Jean-Christophe and Raoult, Didier et al. 2020. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. International Journal of Antimicrobial Agents. March 20, 2020. https://www.sciencedirect.com/science/article/pii/S0924857920300996.
Risch, A Harvey. 2020. Early Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis. American Journal of Epidemiology. May 27, 2020. https://doi.org/10.1093/aje/kwaa093.
The National Institutes of Health COVID-19 Treatment Guidelines Panel . 2020. Coronavirus Disease 2019 (COVID-19). covid19treatmentguidelines.nih.gov. April 20, 2020. [Cited: May 1, 2020.] http://archive.is/gk3xt.

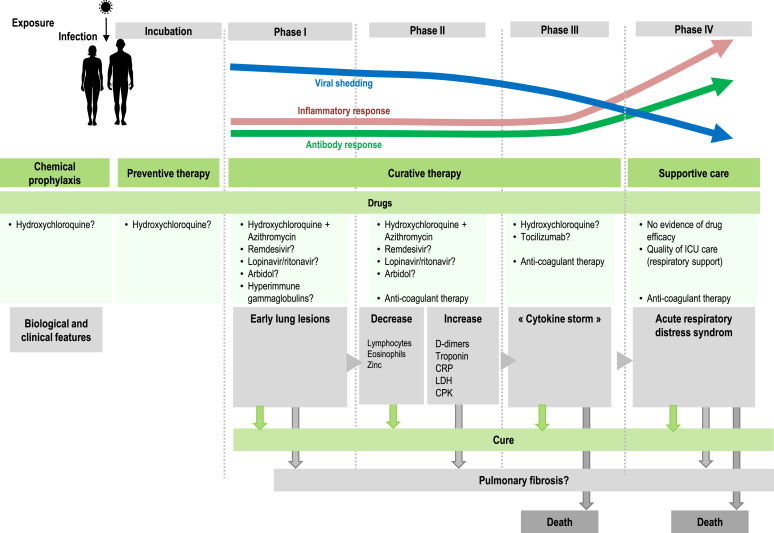 The evidence is mounting from frontline caregivers dealing with Covid19 patients. Previous posts provide examples of HCQ treatment along with other proven medicines (eg. Azithromycin) and supplements (eg. Zinc. vitamins C and D). Summarized in the chart above is the role of HCQ+ according to the progression of the disease Covid19.
The evidence is mounting from frontline caregivers dealing with Covid19 patients. Previous posts provide examples of HCQ treatment along with other proven medicines (eg. Azithromycin) and supplements (eg. Zinc. vitamins C and D). Summarized in the chart above is the role of HCQ+ according to the progression of the disease Covid19.